

The Canada Health Accord ceased functioning on March 31, 2014. There was no state funeral. The Accord was negotiated in 2004 under Prime Minister Paul Martin and set up the last ten years of funding and health care service delivery agreements. Cash transfer increases of six per cent annually ensured the provinces a steady cash flow to build public health systems. The 10-year Plan to Strengthen Health Care ruled until the Conservatives captured a majority in 2011.
Like mad farmers thrashing implacably at wheat, the Harper government cut $36 billion from health care beginning after the 2015 election instead of renegotiating the terms of the Accord when it expired last month.
Meanwhile, parties bent on privatization have acted subterraneously, allowing all sorts of dangerous privatization at the margins of health care — from long-term care to user fees to private clinics — pushing down the quality of health care and sullying the notion of universality.
A piece by Ruth Hubbard and Gilles Pacquet instructively outlines how enemies of public health care agitate for corporate pirates. In a recent How Ottawa Spends the two shadow Von Hayek’s notion that policy-makers are inescapably ignorant of all the social variables at play and markets — information in the form of scarcity prices — will serve as a corrective. They, I submit, are the ignorant ones.
Audacious claim
Exhibit A: “Except in trivial circumstances, the public process is at best a matter of trial-and-error that must routinely fail.”[1]
Saying there is a lack of information for policy-makers in 2013 is an audacious claim, given that the Harper government’s broadside of the National Aboriginal Health Organization and the Health Council of Canada in 2012. Now defunct, both bodies dedicated to cross-country equity collected vast troves of information on public health available to inform the decisions of practitioners, policy-makers, families and individuals.
Hubbard and Pacquet argue against the Canada Health Act (CHA) 1984,[2] which is distinguished as a “goal-and-control” system that “generates steep cost increases (circa eight per cent per year, i.e. at a pace higher than the growth of the GDP), quality that is patchy and not comparatively good overall” (182). For Hubbard and Pacquet, goal-and-control leads to obsession over indicators like wait times or the budget and focuses while the fundamental underlying contradictions go unmended. There is inelastic demand for health, they argue; that is, the cheaper we make it, the more people want it. She gives evidence that for every rise in family income by one per cent, health care consumption rises by 1.6 per cent.
After basing their economic arguments on studies from guys that hang their hats at the ignoble Fraser Institute, they argue the biggest challenges to health care sustainability are collective action and the notion of citizens of basic health service as a ‘sacred right’:
-
A CHA that prevents the demand from being satisfied by private/not-for-profit providers paid for by private citizens
-
the assumption that citizens have a sacred right to receive “basic” health care services free from the public sector monopoly;
-
the immense power of corporatist groups that prevents the modification of the production process; and
-
a general failure of accountability in the whole system
It’s easy to test if the guidelines for Hubbard-Pacquet reform would hold up. We can look at the long-term care sector in Ontario, which is outside the CHA, is dominated by private interests and where corporatist interests (read: union power) have been partially rolled back. If this is what they think the health reform ought to look like, I think we should all steer clear of their advice.
Privatization, reform and Ontario’s long-term care sector
Beginning in 1995, then-Premier Mike Harris sent 6,000 nurses packing, cut 28,000 health-sector jobs in all, closed about 28 hospitals and abolished the legislated minimum standard of care in long-term care homes, which was 3.5 hours per resident per day. This standard was a baseline measurement and some residents need way less and some need way more. Ontario is the only province without this regulation, a legislated minimum standard of care, which a major 2001 study from the Centre for Medicaid and Medicare Services (CMS) concluded that below 4.1 hours is a dangerously inadequate staffing level for the care process needed for the furtherance of independent, daily living. Ontario has been moving in the dead opposite direction.
In came private long-term care homes and American-style managerialism in a sector which resisted this style of control to the hilt traditionally. Forty per cent of Ontario long-term care beds were built since 1998 and constructed based on a competitive bidding process.
Staffing levels were pushed so low that the system has become dominated by chemical and physical restraints, like strapping residents down and doping them up without consent. Naturally, this has led to obscene rates of homicides as heavy care patients have been downloaded into facilities poorly equipped, understaffed and under-trained.
Between 1998-2001 there were 11 official homicides. One of the most grim of all occurred in North York when, as Colin Freeze put it, “Piara Singh Sandhu, 74, had been checked into the home for only a few hours when he grabbed a piece of metal and bludgeoned to death two men, Ezzeldine Elroubi, 71, and Pedro Lopez, 83.” After the brutal slayings at Casa Verde near York University, the coroner’s inquest released in 2005 outlined necessary steps needed to stop preventable fatalities and homicides. This included a minimum standard of care. Today, health-worker unions argue for the full implementation of the coroner’s report.
Dalton McGuinty tore into office in 2003 with a mandate to restore peacefulness with teachers and healthcare workers. Health Minister George Smitherman promised a ‘revolution’ in long-term care. Yet the system of ‘competitive bidding’ set up by the Community Care Actions Centres, which have survived almost 11 years of Liberal governance, has heavily favored for-profit nursing homes. Only two months ago did Bob Hepburn print about hefty salary raises over the last five years for CCAC boards, which has risen by 30-50 per cent in some cases since 2009.
The McGuinty-Wynne governments, like the Harris-Eve regime, opened the gates for shabby corporate care. By the end of the PC era in 2003, U.S.-based Real Estate Investment Trusts and management consultants controlled the lionshare of the 18,800 new beds built, 3,500 redeveloped and 5,000 beds still under construction. They were collecting public subsidies as licensees of the government, while jacking up the rent residents pay as a form of user and resident fees.
The McGuinty government hired 6,100 front-line staff, including 2,300 nurses and opened 7,712 LTC beds between October 2003 and July 2007. Behind these inadequate commitments, nurses organizations and resident groups continued to clamour for better standards as Ontario sank to dead last in many common performance indicators for nursing home care. Despite promises for a standard, the McGuinty government proved to be snakes in the grass. Their Long-Term Care Act introduced in 2007 was called ‘window dressing’ at its arrival and gainsaid a promise that Smitherman had earlier made to health-sector workers to have a minimum standard.
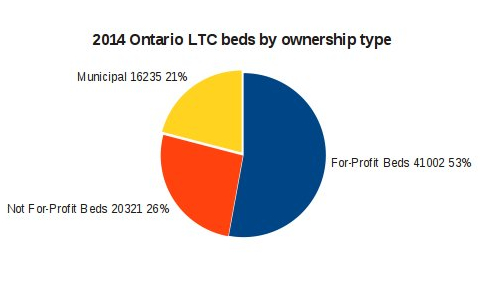
Table 1: author’s calculations, taken from the MOHLTC website.
Homicides continued unabated. Between 2001 and 2010, there were 25. There have been 53 Canadian-wide since 1990. ‘Accidents’ are not included, such as lethal doses of pills or falls or else the number may be higher. There has been a sharp uptick in resident-on-resident violence too. A May 2012 report from the Long-Term Care Task Force on Resident Care and Safety outlines that 1,568 of 2,773 cases categorized as ‘abuse/neglect’ were from another resident’s hand. CTV’s W5 recently did a report on homicides entitled “Crisis in Care.”
Currently, the Liberals are building 3,500 beds per year as part of a ten year/35,000 bed plan. Since 2008, there has been a 29 per cent increase in RPNs in Canada. But the government can’t keep up and its ability to monitor the long-term care sector appears dubious. During the implementation phase of its Long-Term Care Act, which saw an Ombudsman SORT investigation,Wally Baker, in Leisureworld-O’Connor in Toronto, was found dead in his physical restraints. Florence Coxon died from her wheelchair restraints just three days prior.
The problems are piling up. As Thomas Walkom recently reported, between 2005-2012 median wait-times nearly tripled from 36 to 98 days, despite George Smitherman wildly sobbing and promising revolutions. Nursing home capacity has hardly increased. Fifteen per cent die on the waitlist, those who make it in die within three years of admittance.
The waitlist has virtually exploded, an 85 per cent increase between March 2005 and March 2012. The beds have increased by a mere three per cent. Part of the waitlist mitigation strategy of the McGuinty government was to make eligibility criteria more strict, which helped the government decrease the amount of people waiting by 15 per cent. But where have they gone?
Why has bed capacity expanded so feebly when the government has committed funding? Walkom explains it by the quick rise in ‘preferred accommodations,’ which are about $2,200 a month for the deluxe. Those that can pay get inside, while standard accommodations remain brutally competitive. Walkom argues 40 per cent of beds in the province are standard beds and 60 per cent on the waitlist are requesting them. Since accommodations isn’t under the umbrella of ‘care,’ the rent goes straight to the shareholders. Resident fees vary widely across Canada, from $32 to $102 a day.
In industrialized long-term care, the axioms of the CHA have no sway and corporate care has dominated the field where grotesque stories of neglect are common. Unregulated personal support workers (PSW) are increasing, with some 90,000 tending to clients as best they can, but with Alzheimer’s on the rise and the Ontario government desperate to save loonies, there is a lethal contradiction at play. The number of people with Alzheimer’s in Canada is expected to rise to 1.4 million by 2031, up from 750,000 today.
Based on the performance of long-term care reform in Ontario, Ruth Hubbard and Gilles Pacquet’s prescriptions for more privatization and shredding the CHA generally seem batty and dimwitted.
The future of health care
One of the first studies of public health in London was done by Friedrich Engels, who remarked that “under capitalism, social warfare is waged with the weapons of the means of production and subsistence and the collateral damage is suffered by the poor.” As a general principle, this still holds. According to recent studies, the savagery of economic competition is exposing workers across the occupational spectrum to a range of physical work hazards and psycho-social health risks related to work, worklessness and unemployment. Low reward, low control, and injustice at work has been linked to increased risk of coronary heart disease. Clare Bambra, for instance, has shown that adverse psycho-social risks are higher at the bottom end of the job market where repetition, tight deadlines, monotonous, machine-paced work is more prominent.[3]
Robert Chernomas and Ian Hudson, in their new book, To Live and Die in America, put the tedious debate over the aging society in context. This era of capitalist development is the chronic condition phase, as opposed to the infectious disease phase that characterized the industrial revolution up to the turn of the century 1900. Since then, life expectancy has expanded mainly through surviving birth and public health initiatives, health and safety boards and committees, improvements in diet and hygiene and, most importantly, rising wages. Yet the infirmities arising from exposure to Fordist and post-Fordist forms of work and workfare states are leaving people living sicker, with higher degrees of acuity, up and into their 1980s and 1990s, with no national strategy for long-term care, dementia or mental health in Canada’s context. The privileged can pay for care, the poor can’t without pauperizing themselves.
Health inequalities are spreading across Canada like mustard gas. By the Harper government’s hand, things are only slated to get harder for working and workless people to access affordable health services. A little-regarded reform of December 2011 was the squelching of the equalization formula built into the Canada Health Transfer — Canada’s largest major transfer from the feds to the provinces. The formula of PM Martin’s CHT (Canada Health Transfer) was that the ‘have/have not’ category factor in to the funding calculations, along with income tax point transfers.
Marchildon and Mou explain that under the Martin CHT, “when computing CHT cash transfer, the income tax point transfers of the provinces are firstly equalized up or down (in the case of Ontario) to the national average, and CHT cash transfer are then calculated as a residual of the equalized tax point transfer. Under this formula, all the have-not provinces receive a CHT cash transfer of $923 per capita.”[4] Now, there is no more block funding in the fed-provincial health transfer, which originated in 1977. Ultimately, all provinces except for Alberta will be losers. Forty-eight years after Medical Care Act of 1966, the Harper CHT will begin this year.
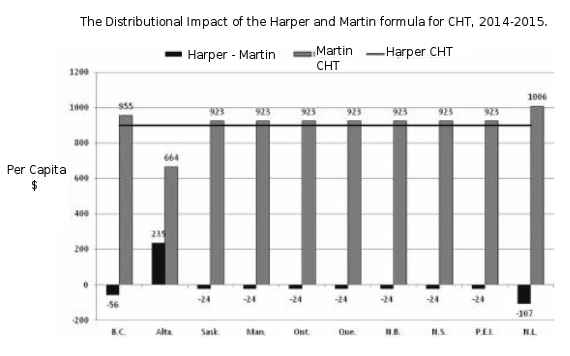
Table 2: taken from Marchildon and Mou.
Most likely, the fiscal position of the feds will improve and that of the provinces will deteriorate. Downloading will not cease. Harper’s policies are lethal and the perfidy ought to be resisted root and branch. It’s eyes wide shut to violence and missing and murdered Aboriginal women while life expectancy for First Nations men in Toronto is 37. The Harper Conservatives, “Canada’s Founding Party,” are double-dealers drenched in colonial bloodstains. This colossal colonial failure is unjust and a public health catastrophe.
Yet, there are many tactical options to renew public health care.
-
Support the drive for a minimum standard of care in long-term care
-
Support for funding, space and autonomy to deal with the First Nations public health crisis including support for a national inquiry into missing aboriginal women
-
The development of a national plan to comprehensively train, pay higher wages for PSWs across the country and the design and implementation of support mechanisms for informal care givers. (The Ontario Minister of Health has agreed to raise the wages of PSWs to $16.50/hour by April 2016. An SEIU campaign!)
-
The ending of inappropriate anti-psychotic drugs in nursing homes
-
The public recognition that care-work is primarily women’s work in order to eliminate gender bias in labour market trends in health care
-
The democratization of Health and Long-term Care ministries and the Local Health Integration Networks (LHIN) system including full public participation in knowledge and decision-making
In many cases, these movements are already in train and despite governments inhibiting their development, they continue, slowly but steadfastly gaining ground.
Justin Panos is a freelance journalist. Follow him on Twitter at @justinpanos.
Endnotes:
1. Ruth Hubbard and Gilles Paquet, “Public Policy as an Inquiring System: The Case of Canadian Health Care” in (eds.) Christopher Stoney and G. Bruce Doern, How Ottawa Spends, 2012-2013, The Harper Government: Mid-Term Blues and Long-Term Plans, McGill-Queen’s University Press, 2012, p. 173.
2. The Canada Health Act outlines the five pillars of medicare: Universality, Portability, Comprehensiveness, Publicly Administered and Accessibility.
3. Clare Bambra, Work, Worklessness, and the Political Economy of Health, Oxford University Press, 2011, p. 92.
4. Gregory P. Marchildon and Haizhen Mou, “The Conservative 10-Year Canada Health Transfer Plan: Another Fix for a Generation” in (eds.) Christopher Stoney and G. Bruce Doern, How Ottawa Spends, 2013-2014, The Harper Government: Mid-Term Blues and Long-Term Plans,
The article originally appeared on The Socialist and is reprinted with permission.
Support rabble today!
We’re so glad you stopped by! Thanks for consuming rabble content this year.
rabble.ca is 100% reader and donor funded, so as an avid reader of our content, we hope you will consider gifting rabble with a donation during our summer fundraiser today.
Whether it be a one-time donation or a small monthly contribution, your support is critical to keep rabble writers producing the work you’ve come to rely on as a part of a healthy media diet.
Become a rabble rouser — donate to rabble.ca today.
Nick Seebruch, editor

