The worst outbreak of one of the most deadly viruses, Ebola, is occurring in a corner of the world generally ignored by the rest — the intersection of Guinea, Sierra Leone and Liberia. Medicine Sans Frontiers, says it is in a race against time to curb the epidemic. Having lived and worked in Kailahun, the centre of the affected region, I would say Ebola had 20-30 years head start.
Since March, over 1,300 people have been infected and 870 have died from Ebola. Until the virus spread to neighbouring Nigeria, fueling fears it might reach the West, there was little media coverage of this epidemic. What is published equates the outbreak with traditional beliefs, poor governance and more subtle versions of ‘these things happen in Africa’. But it’s not culture, ignorance or even geography that lets Ebola run rampant. It’s a history of conflict and underdevelopment.
The first time I traveled to Kailahun, in 2010, I was told, “this is where the war began, and the last place it ended.” Sierra Leone’s civil war lasted from 1993 to 2003. Throughout Kailahun was the headquarters of the Revolutionary United Front, the rebel militia, which became famous for the forced conscription of child soldiers and chopping off of limps.
Since the war ended, women and children have returned from refugee camps to rebuild homes and reclaim farmland. Former child soldiers have become motorcycle taxi drivers. Organizations like SEND, which I worked for, are supporting development by forming credit unions and offering agricultural support. But Kailahun remains one of the poorest districts the country, and Sierra Leone remains one of the poorest countries in the world.
The District Hospital in Kailahun — the primary health facility for the 600,000 people — is staffed by one doctor, and often short on medicines, clean water and electricity. The hospital boasts a new operating room, used mostly for cesarean sections; Kailahun had one of the highest maternal mortality rates in the world. It also has a feeding center for malnourished babies; Kailahun also has one of the highest infant mortality rates. When I was there, I witnessed near weekly parades of wailing women, carrying tiny corpses to the river to be washed, an honor traditional practice dictates for the dead.
This is the scene Ebola entered: a context already ripe with poverty and ill health.
An email from my colleague in Kailahun reads, “We’ve dealt with armed conflicts and natural disasters but not a virus without cure.” A number of the women involved with SEND have fallen victim, as well as nurses in SEND’s Health Sector Governance Program. SEND closed its usual projects in May, and has since been working with other organizations and the government to provide education about the virus.
These sensitization programs are as essential as any medical service. Some communities are attacking health workers, refusing to let them remove the ill and dying. SEND reports, “Frequently, the taskforce and surveillance teams are prevented from taking blood samples of suspected patients for testing at health facilities. The ambulance service for Ebola cases has been prevented from entering some communities… the ambulance team was assaulted and the windscreen of the vehicle vandalized.”
After local health workers fell ill, rumors circulated that they spread the virus. Without basic supplies, such as gloves, there is high risk that health workers may contract and share the virus, somewhat justifying these fears.
When foreign medics arrived they banned the traditional washing ceremonies of the dead, as this increases risk of infection. Instead they demanded bodies be bagged and put in mass graves — an obscene act of disrespect in local culture. The coinciding arrival of foreign medics, with more visible signs of the virus (such as isolation centers for the ill) caused people to question if it is actually the foreigners and their strange ways, which caused Ebola.
It’s not surprising that there is a lack of faith in foreign medical professionals who have been absent for decades of war and malaria, and now show up in hazmat suits because they are scared that the virus might spread — that people other than those in remote villages might fall ill and die.
Communities struggle to understand public health practices of quarantine. The education required to comprehend viruses and contagion cannot be provided in an instant, during a terrifying emergency. It requires time, the building of knowledge — a luxury in a community were only 20 per cent are literate, and most teenagers don’t finish school.
Despite these historic challenges, and continued reports of a growing epidemic, I believe the situation will improve. Local leaders are mobilizing education campaigns. Traditional chiefs are speaking out against attacks on health workers. Together with organizations, they are coordinating door-to-door sensitization discussions. As Kim Yi Dionne notes, applying local knowledge and practices is often the most effective approach in a health crisis.
In the race against the epidemic, the playing field is titled against the people of Kailahun, as it’s been during crisis for decades. It’s only by correcting this unbalance that this, and future, health crisis can be addressed.
Julia Smith is a community/international development and research consultant, specializing in issues related to human rights. She is currently completing her PhD in Peace Studies at the University of Bradford and is based in Vancouver. @juliaheather
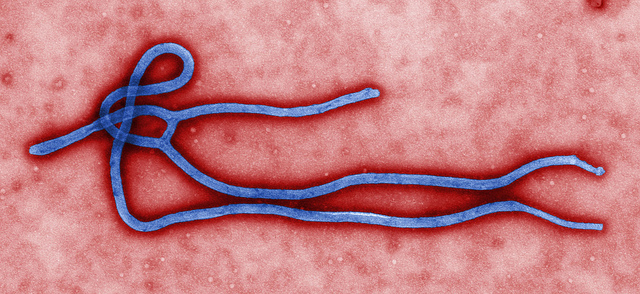
Photo: flickr/Global Panorama
Support rabble today!
We’re so glad you stopped by! Thanks for consuming rabble content this year.
rabble.ca is 100% reader and donor funded, so as an avid reader of our content, we hope you will consider gifting rabble with a donation during our summer fundraiser today.
Whether it be a one-time donation or a small monthly contribution, your support is critical to keep rabble writers producing the work you’ve come to rely on as a part of a healthy media diet.
Become a rabble rouser — donate to rabble.ca today.
Nick Seebruch, editor

